Doctor First Appointment system – A 21st century Solution?
“Accept the things you cannot change, and change the things you can”
– Reinhold Niebuhr
No one can argue that current ‘demand’ in the NHS is high.
We can argue until the cows come home, as to why, or who/what is responsible for this ever increasing demand. But unless we think we can alter this demand in the immediate foreseeable future, maybe – just maybe – we should start thinking about how we can manage it.
What if it is time to adapt?
For more than 60 years now – long before the birth of the NHS – General Practitioners have been offering the same traditional style of service: Patient decides on need to see doctor. GP offers a time to be seen. GP sees patient.
This has always been considered the gold standard, the very essence of the much coveted doctor-patient relationship, in UK primary care.
But it is reasonable that this traditional style hasn’t really evolved with an ever changing 21st century National Health Service? Are we clinging on to the past too much?
“All great changes are preceeded by chaos” – Deepak Chopra
In February 2013 our NHS GP surgery embarked on a new kind of appointment system known as “Doctor First”.
I can only write about my personal experience, the highs and lows. It is my own views which I express, and not necessarily those of my partners. Other practices may have very different experiences. I will try and update this blog monthly, to let you know how things are progressing, and if we are surviving! (The updates will be much shorter. Honest)
There are several similar systems to this being implemented Nationally, ‘Doctor First’ is just the brand-name of one such system. Others I know of, which work in a similar vein, are ‘Patient Access’ and ‘The Stour Surgery System’.
I’m sure there are more, but as I have no experiences of these other systems, I cannot comment on the similarities, or differences, between them.
It’s only early days for us, and we have a lot to still work out, but I’ll try and précis the gist so far.
How we got here:
We are a very busy sub-urban Practice, on the outskirts of Middlesbrough, with 4.25 whole-time equivalent GP’s, covering a list size of 7,300 patients. We have one Nurse Practitioner, and no salaried GP’s.
Over the 20yrs that I’ve been in the Practice, we have changed the appointment system dozens of times. We have desperately tried anything suggested in a quest to find a system that works for both patients, and doctors. We never have.
As a team, we are devoted to our patients. Sadly, this is not always obvious to them, as our appointment system has too often let us down.
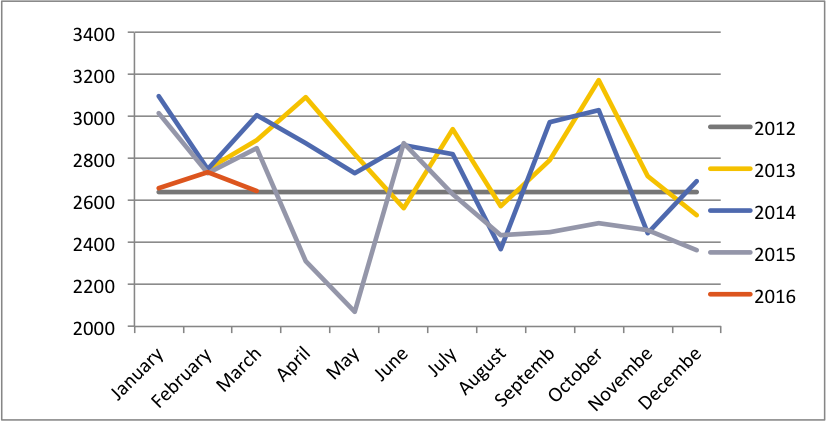
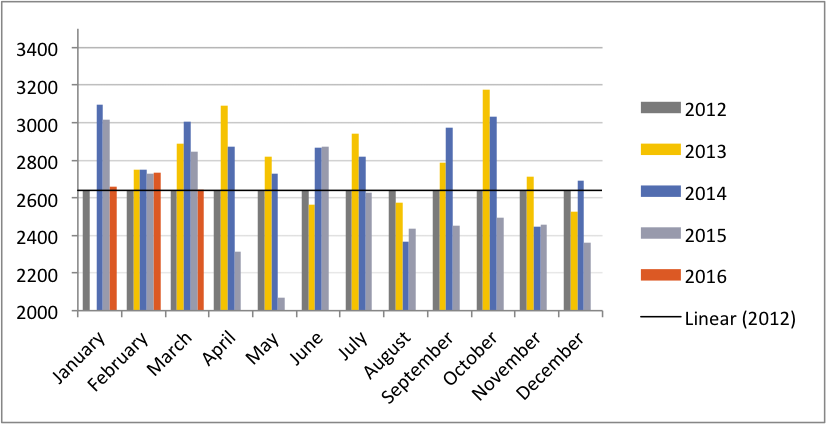
We have always been convinced that we have extremely high patient demand. We now have the data to confirm this belief.
Over the last 15yrs, we have lost 10 GP partners. Four of these were as a direct result of work stress, two left through physical illness, and four were enlightened enough to get out before the workload had chance to get them down! This high GP turnover has only served to compound our workload problems.
Previous appointment system:
Our most recent previous appointment system offered a mixture of same day ‘routine’ appointments, 48hr to 2 week ‘book-ahead’ appointments, and a ‘duty’ GP with reserved appointments every day, to see same day ‘urgent’ requests.
No patient, with a problem they reported as urgent, was ever turned away. We have always had a very low patient attendance rate at A&E or Walk-in-Centres.
What we did have, was patients who were very unhappy with the system. The usual 8am phone jam was a huge source of stress to them, and our receptionists. Many patients couldn’t get through, and gave up. Too often we never even knew who they were. Many were told that all ‘routine’ appointments were taken, and requested to ‘try again tomorrow’. The complaints about the system were high. The receptionists, who took the verbal abuse on the frontline, had very low morale.
We had no choice but to do something different. We had very little to lose.
I can’t pretend it wasn’t scary. We were terrified.
It took an enormous leap of faith. To take down all barriers? To allow every patient to choose who, when, and how they are dealt with? To agree to see everyone of the day they call?
Were we totally mad?
The First Steps:
After 4months of training, planning and education of staff by the Doctor First team, we eventually felt ready, and went ‘live’ on 1st February 2013.
The first stage of the Doctor First system is called ‘Clearing the backlog’. This is to ensure, that at the point of ‘going live’, there is no outstanding, hidden demand, in the form of frustrated patients waiting to be seen.
This stage was pretty easy for us. Our advanced booked appointments were a maximum of 2 weeks ahead, so we had to stop advance booking of appointments for 2 weeks before D-day. Then we had to see everyone who rang in and requested an appointment, in order to clear any outstanding demand.
For these two weeks, all partners worked pro-rata 10 sessions (FTE) and we brought in 4 locum sessions each week, to help.
It was the easiest two weeks of my career. We were so over-doctored!
‘Doctor First’ – How it works:
All nurse and phlebotomy appointments go through a receptionist booking procedure as usual. Any patient who phones requesting ‘GP advice’, or a ‘GP appointment’ goes through the DF system.
The basic principal of DF is that the most senior clinician is the first point of patient contact. It is important to stress here, that the system works entirely on the patient’s choice – with regard to who they see, how they see them, and when they see them. They really have very little to complain about now! Basically we endeavor to give them whatever they ask for. Sounds crazy, and very alarming, but there is some intuitive logic to it, as I’ll go on to explain later.
At very least, they get instant (almost) access to a GP for advice. This has an immediately calming/reassuring effect. Early on in the patient’s journey, they have already reached the person they most wanted to talk to, and this achieves an early sense of security.
Any patient phoning requesting medical input of any kind, gets same message: “Of course. Which doctor would you like to see?”
For continuity, if they have previously been seen for the same problem, they are encouraged to see the same doctor, or Nurse Practitioner again, UNLESS of course, they prefer not to due to dissatisfaction for example.
They are then asked for a contact number, so that the doctor can prioritise, and deal with the most needy, quickly and efficiently. They are also asked if there are any times in the day which would not be convenient for the doctor to call them back. They are told not too worry if it takes time for the GP to call back, as they are guaranteed to be seen that day if they want.
When we call back we ask about the problem, and if appropriate give brief advice, before asking what time they’d prefer to come down. By this stage, 60-70% have already decided they don’t need to come down – they are happy with advice, a sick note or a prescription. Others are directed to alternative community healthcare services. At the end of the telephone chat, if – and only if – both the GP and the patient, are equally happy, and in agreement that they don’t need to be seen, then, end of.
We listen out for non-verbal telephone-cues suggestive of ‘red flag’ signs – pauses, hesitancy in agreeing to telephone advice, apparent lack of confidence in the advice, or a slight pause when asked at the end if they are happy with the advice. Any of these signs – or if they ask to be seen – they then get offered a same day appt. No questions. They are offered an appointment later that day, at a time which suits them. Our appointment availability is such that they can nearly always pick and choose a slot time.
The call has to end with both the patient and GP entirely comfortable with the situation. This is fundamental to the success of the system.
If an appointment is required, we encourage them to come down and be seen same day, but if they prefer another day, we ask them to phone back on the day they want. They can remind us we’ve already discussed the problem and we’ll agree a mutually convenient time on that day. This method allows for unexpected eventualities cropping up in their lives, or that of the GP, thus avoiding DNA’s and cancellations. The same applies if they want to come down another day after work/ day off etc. We agree the time on the day.
If they really want/need to prebook a specific time – we let them. But this is surprisingly rare in our experience so far!
Advantages and Disadvantages.
For ease, I will break these down into Patient, Doctor and Receptionist advantages and disadvantages, but you will see there is much overlap – and advantages can also be disadvantages and vice versa!
Advantages:
The advantages for the patients are fairly obvious. They get appointments (or advice) fast, and at their convenience. They get continuity of care. If they are complex or ill, they get more time with the GP, and so a more holistic package.
If they are working, or have children’s school commitments, we can agree to see them before school finishes, or after work in the early evenings. We try to be pretty flexible, within reason.
On a daily basis, we get comments “thanks for seeing me/dealing with me so quickly”. The feedback so far is very encouraging.
The advantages for the GP’s are that we are more in control of our workload. We can book the right people in for the right slots. We can work more flexible hours (no such thing as an am/pm surgery any more) and can fit the appts in around visits/paperwork/meetings/coffee breaks etc. We are seeing far less patients face-to-face, but at least we know we are seeing the needy ones. As a result we can give them much more time and deliver much better quality medicine. Each GP ‘sees’, around 10-12 patients in a day since we introduced this new system. Many are children who just need a 3-minute safety-net consultation, the rest are the complex patients, with potential red flag symptoms. The latter can be spaced at 30-40minute intervals so we have ample time to take a really thorough history, examine, dictate a referral, speak to the local hospital consultant, or whatever is required, all whilst the patient is still sitting next to us. A package of care is agreed, hospital advice or clinic reviews are arranged, and all in one sitting. It’s wonderful. I have spoken to more consultants on the phone in the last 4 months, than I have been able to do in years. The tailored packages of care that result from this, are a refreshing breakthrough.
It’s also much easier seeing/speaking to patients who have requested you by name – these patients, or their problems, are already well known to you. They already trust and have confidence in you. Consequently, they are more prepared to accept telephone advice, and in turn, if the GP knows the patient well enough to be aware of their limitations, he/she is more comfortable giving that advice.
The advantage to the receptionists is that they have no more confrontational battles. Within a couple of months of the new system, we saw a complete transformation of the receptionists. They became again, the happy, smiley people we had once employed, now relaxed and released from the wrath of complaining, and understandably frustrated, patients.
Sadly, this rosy glow was not to last long as other issues arose.
However, their roles are now released freed-up time to do more administrative work/QOF data trawling, and thus allowing the GP’s to stick to being ‘clinicians’.
Disadvantages:
To the patient. Not many. At the time of writing, we are 4 months into the system, and we have no formal/major complaints yet. (We were use to dozens a day in the previous system, complaining about the phone lines, or that they couldn’t get an appointment). Most of the patient chatter in reception is very positive and encouraging.
Theoretically some similar systems have apparently given rise to patients complaining they never get to actually ‘see’ the doctor. As mentioned above, if they want to be seen, that’s an indication to see them.
We’ve had a handful expressing minor concern at how long they’ve had to wait for the doctor call back on occasions. We hope in time, when they are more confident in system, this will be less of an issue.
One patient has mentioned that they ‘do not like answering the telephone’, but these sorts of issues can be discussed and resolved on an individual basis.
Contrary to the beliefs of some, Doctor First doesn’t discriminate against people who are not good on the phone, for whatever reason. These patients will be identified by themselves, or by the GP, and will simply get offered, or choose, a face-to-face appointment. However, it is true that the success of the system does indeed depend on having a majority of patients who are happy with telephone consultations. I can imagine this would present inherent problems in a Practice with a high population of non-English speaking patients.
The disadvantages to the GP.
It IS hard work. For the GP’s, the work is undeniably intense.
By lunchtime, my eyes are sore from staring at the PC EPR/appts screen.
Whilst the mornings are hard, the afternoons usually lighten up.
Doctor First Data repeatedly shows that 2/3 of a GP’s workload comes in before midday. So, although tired by 1pm, you’ve pretty much cracked the day.
At least you don’t have to embark on an 18-patient face-to-face afternoon surgery, at a time when you are already tired, and the consequent struggle to keep everyone to their 10minute slots. Doctor First suits my tired afternoon brain – I always struggled with the p.m. surgery, and worried how safe I was.
I’ve usually spoken to around 30-40 patients by 1.30pm, but may have only seen 4-5 of them.
Despite this, it doesn’t really feel like working in a call centre, as some have suggested, because the patients to whom you are speaking, are well known to you. The conversations are, therefore, very comfortable.
When all GP’s are in, I’ll speak to about 10-15 more people in the afternoon and see another 4-6 (some of whom were booked in the morning but requesting an after school slot).
During GP leave periods, it’s a different matter.
The demand for clinical input remains constant regardless of any reduction in workforce. These spells provide the biggest challenge. The same volume of calls are shared amongst fewer GP’s. Making up to 70 clinical decisions a day is hard, and the days are long.
Over the Easter holiday period, and for a couple of weeks since, when GP Partners were off, I have been working 14hr days, and have been beginning to wonder if this really is sustainable. That said, 12hr days were the ‘norm’ for me in the old system, and 14hrs were not unheard of during busy spells. Such times are always challenging – for any system.
Another Practice, piloting Doctor First locally, admitted that whilst hard, they still find holiday cover less stressful and less demanding than their old system – despite a lower patient demand than ours. I’m inclined to agree.
One thing we have all noticed, however, is that we are becoming more ‘conditioned’ to this style of working, and are finding it becomes easier as we get more experienced at it.
The disadvantages to the receptionists
. This is really interesting. We didn’t anticipate any of these at all, but a couple of problems have been highlighted.
The major problem we are currently facing is the late finishing time at the end of the day. In these early weeks, whilst everyone adjusts to the system, the doctors have frequently been working late, and bringing patients down long after the receptionists day is due to end. This is particularly a problem when the workforce is down through GP absence. It has resulted in the need to pay overtime for those staff members willing, but others have been reluctant to stay back. Commitment, loyalty and a vocational sense of duty is proving an invaluable quality here. However, this is causing a rift in the team, and we have safety concerns to consider if reception staff are unable to stay back until all patients have left the building.
We are currently working on solutions that are acceptable to all, but it’s not proving easy.
On a lighter note, the Office Manager has reported that receptionists are starting to feel a bit ‘lost’! They feel their skills and training are not being used to their full advantage. They are keen to have some control back and use their own sensible judgements for certain ‘clinical’ requests, such as, for example, same day prescription requests. Currently, all clinical requests are directed to the doctors, so this may indeed need tweaking a little.
The funding issue /CCG /Private company support
I am often asked if we really needed to employ a private company like DF, or could we just have done it by ourselves? In all honesty – I don’t think we would have embarked on this, nor succeeded, without the support of Doctor First. They seemed to know and pre-empt all the pitfalls, but more importantly held impressive and reassuring data on other Practices who had done it and survived! Without that reassurance, I don’t think we’d have ever had the confidence, or the necessary understanding of the system, to take the plunge.
Middlesbrough PCT, now Middlesbrough CCG, invited several companies to tender bids, and present their case. As a result of this process ‘Doctor First’ were selected.
Given that the PCT /CCG were offering to fund it, the decision to proceed was a no-brainer for us. We had nothing to lose. If we’d had to fork that money out for ourselves, I guess, if I’m honest, we could never have justified the cash to do so. However, we now regard it as money well spent.
The practice have incurred small financial costs (such as additional locum sessions in the preparatory 2 weeks), but larger time investments – especially in the preparatory weeks when partaking in data collection, training, logistics & solutions meetings with the Doctor First team. A lot of this time however, can now be off-set against the time no longer taken for dealing with complaints from regarding the old appointments system!
The Doctor First team have inspired us, helped us, re-trained (and re-motivated) our reception team, and taught us a great deal about patient demand/appointment systems along the way. They have provided us with some really useful data.
I think one of the most important aspects we have learnt, is to run with their expertise and advice – no matter how counter-intuitive it has felt at times! on occasions, it has been very hard to resist the temptation to alter things slightly. One of the first 3 practices in our Middlesbrough pilot has now pulled out. I have been told, that very early on – they adapted the system to what they thought they needed. It didn’t work.
The one thing that has amazed us all, is just how accurate all the Doctor First forecasts have been. Everything they said would, or wouldn’t, happen has been just as they predicted. We have started to realise just how predictable patient consultation rates are over a working week. Our only gripe, is that they advised us to use their own ‘standard data’ rather than the data we collected, as they believed our data may not have been collected accurately. They assured us their data had proven reliable in multiple practices. We rearranged our working patterns to ensure our weekly GP-sessions covered the predicted demand for each day. It turned out, as we expected, that our patient demand was higher than average for comparable practices. The minimum GP sessions advised by Doctor First, turned out to be not enough.
Doctors First believe they can give accurate demand predictions, almost day-by-day, for every month in the year. To the extent, for example , they believe they can accurately predict, what our appointment demand will be on the Wednesday before Easter, 2015!! Fascinating stuff.
The drive for the PCT/CCG is to improve patient access and services, and reduce the load on Walk-in-Centres, and A&E, which was thought to be created by GP-appointment overspill. It will be some time before the data is available to confirm whether this ambition has been realised. Middlesbrough, had very poor patient access survey results. They initially offered funding to 3 Practices prepared to pilot this, with a pledge to fund all others if successful. To date, 8 Practices in Teesside have now “gone-live” with 4 more practices signed up and preparing. It will be interesting to see how we all fair over the next 6 months…
The future:
Doctor First data suggests that nearly all their Practices have reduced the number of sessions per full-time equivalent, because they are working so much more efficiently. This they argue, frees up time for alternative income generation, or new service provision. Personally, we are along way off seeing this yet – it remains but a pipedream!
The role of the Nurse Practitioner is proving more worthwhile than ever. Many of the patients who are most difficult to assess on the phone, are the very patients that fall within her remit – rashes, throats, ears, joints etc.
We always had a problem filling the NP appointment in our old system. Patients would always choose the GP as a first default. In the new system, after speaking on the phone, we can reassure them of her skills and competence to deal with their problem. We are fortunate to have an excellent NP and most are more than happy to see her if we suggest it.
The next aim is to use the freed-up receptionist time and train them in QOF data collection and admin to trawl in income, leaving GP’s freed-up to be ‘doctors’. The Doctor First team hold impressive stats and data on Practice savings/profits through this system. We will see.
Patient education is an extremely important aspect of the system.
Previous health-seeking behaviour patterns of our patients, stem, I am sure, from the inadequacy of our previous systems. By rationing the appointments available, we had ourselves created a sense of urgency and panic.
We hope that in the long term, education and reassurance that patients will be seen when they need to be seen, will gradually start to impact on demand.
Our ‘demand’ figures are very high when compared to similar practices for both size and demographics. Whether this is an historical problem from encouraging doctor-dependency over the years, or whether this is a more specific demographics issue is not clear, but we hope with ongoing understanding and education, we may be able to make a difference to future demand, as the years go by. ….
We will see. All fingers crossed.
One Practice who has been operating a similar system for over 4yrs, recently advised me, that after years of training, many patients were now ‘self-triaging’ and appropriately requesting telephone appointments.
In Summary…..
On a personal note, I certainly feel I’m working much safer now; more efficiently, and more effectively.
At the end of each day, I know I have seen everyone who really wanted to be seen, so there is no going to bed anxious that I’ve breezed over someone simply because I didn’t have a spare appointment to offer.
I also worry, how many vulnerable patients were never known about in the old system. It allowed the strongest, or those with the loudest voice, to get priority. The weakest, most frail, elderly, or quietest would give up at the first hurdle – getting through on the 8am phone-rush.
The new system seems fairer. It is more balanced, both for the patient and the GP.
It no longer depends on which of the two, is feeling strongest on the day. It depends on entirely on clinical need.
More importantly, know I can deliver 30-40mins of high quality medicine to those patients that need it most.
In the old system, large numbers of patients complained that they could never get an appointment. Others were in four times a week seeing different doctors. I still can’t fathom how they managed to work the system with such reliability. The new system ensures that appointments are still availability by mid-afternoon, if a needy non-frequent attender happens to phone up.
On the whole, the doctors feel less stressed and more in control of their workload. They feel more satisfied and relaxed at the end of the day, despite still working long hours.
This is with one exception.
Sadly, we have lost our newest partner, a very competent and caring clinician, through Doctor First.
We took on a new partner a couple of months before we embarked on the new system. Despite them embracing the concept of Doctor First from the outset, and being very much committed – not only to the team, but also to the philosophy of the new system – they just felt it wasn’t for them. After trying desperately hard to make it work for 2 months they still found themselves longing for the old system – in their words “for a ‘normal’ surgery” of 18 pre-booked patients.
Together, we considered lots of options, perhaps whether there was room for a hybrid middle-ground with GP’s opting in or out of the system, but in the end, and with heavy hearts, a mutual agreement to go our separate ways was agreed.
It’s not for everyone.
In particular, I think that newer, junior partners, who know patients less well, are probably at a disadvantage, and of course, there are doctors, as well as patients, who are less than comfortable with telephone consultations. No one hat fits all.
Admittedly the system may seem threatening to those uncomfortable with phone based systems, but patients at least, can be reassured and offered a face-to-face alternative.
Doctor First gives the ability for GP’s to triage priority and be in control of their workload. The old system gave no control, and either poor or no triage at all. Any triage that did take place, began from a negative stand point, once all the appointments had been taken. This traditional kind of ‘triage’, aimed at limiting access once no appointments were left, was very stressful.
Doctor First eradicates the need for patients to ‘game’ the system. Patients do not have to justify whether their problem ‘deserves’ an urgent or routine slot. If you are ill, or need to be seen, you will be – and in most cases by the GP who knows you best.
All in all, it just seems very intuitive. Right for patients and right for doctors… “Put the most senior clinician on the frontline – not the most inexperienced or least qualified.”
This system has potential, but be warned, it’s not for the faint hearted. It requires robust GP’s, and full team commitment to it.
Four months in, and all the pre-existing partners firmly believe it is the best system we’ve tried so far. Whilst it is still far from perfect, and we still have challenges we need to work through, for the time being at least, we feel could never return to the old style system….
Watch this space….. 😉